Matching-adjusted indirect comparison: entrectinib versus crizotinib in ROS1 fusion-positive non-small cell lung cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To perform indirect treatment comparisons of entrectinib versus alternative ROS1 fusion-positive non-small cell lung cancer treatments. Methods: Relevant studies with crizotinib and chemotherapy as comparators of interest identified by systematic literature review were selected for matching-adjusted indirect comparison by feasibility assessment. Matching was based on known prognostic/predictive factors and scenario analyses were used for unreported confounders in comparator trials. Results: Entrectinib yielded significantly better responses versus crizotinib in all scenarios (odds ratio [OR]: 2.43–2.74). Overall survival (hazard ratio: 0.47–0.61) and adverse event-related discontinuation (OR: 0.79–0.90) favored entrectinib. Progression-free survival was similar across treatments, except in one scenario. Conclusion: These results suggested improved outcomes with entrectinib versus crizotinib/chemotherapy and may help to make better informed treatment decisions.
Introduction
Lung cancer is the most frequent cause of cancer-related death worldwide and is usually diagnosed in advanced stages [1]. The most common histological lung cancer subgroup is non-small cell lung cancer (NSCLC), which accounts for more than 80% of all lung cancers [1]. NSCLC can be stratified by histology and genotype and clinical evidence supports consideration of different treatment pathways for distinct subtypes of lung cancer [2].
The development of some of these tumors is triggered by gene rearrangements in target kinases such as NTRK1, NTRK2, NTRK3 (encoding TRKA, TRKB and TRKC, respectively), ROS1 and ALK. These rearrangements tend to be mutually exclusive and usually have a low prevalence (<10%) [3] across tumor types. ROS1 fusion-positive advanced NSCLC accounts for approximately 1.1–1.8% of nonsquamous NSCLC [4–6], is found almost exclusively in nonsquamous tumors [4–6] and is associated with younger age and nonsmoker status [4,7,8].
Currently, targeted therapies are the standard of care for ROS1 fusion-positive, advanced NSCLC and offer both efficacy and safety advantages over standard chemotherapy in the treatment of these patients [9]. Two of these targeted therapies are crizotinib, an oral tyrosine kinase inhibitor (TKI) that targets ALK, ROS1 and MET receptors, and entrectinib, a potent TKI of ROS1, TRKA/B/C and ALK that was specifically designed to cross the blood–brain barrier and remain in the central nervous system (CNS) [10,11].
Although several treatment options are available for the management of patients with NSCLC, no randomized controlled trial has directly compared the efficacy and safety of these treatments for ROS1 fusion-positive advanced NSCLC. As a consequence, it is difficult for physicians to compare differences in outcomes between available treatment options and select the most appropriate for their patients. In this analysis, we performed an indirect treatment comparison (ITC), with the aim of estimating relative treatment effects of entrectinib compared with alternative treatments in patients with ROS1 fusion-positive NSCLC. The primary comparator of interest for these analyses was crizotinib. Other comparators were pemetrexed plus platinum followed by pemetrexed maintenance, an alternative first-line NSCLC treatment, as well as the standard second-line NSCLC treatments docetaxel monotherapy and pemetrexed monotherapy. For this ITC, the key endpoints considered were overall survival (OS), progression-free survival (PFS), objective response rate (ORR) and discontinuation due to adverse event (AE).
Theoretical framework
For many years, treatment of NSCLC relied on traditional chemotherapy, in particular, gemcitabine and cisplatin-based therapy; however, this approach was associated with poor outcomes and OS [12].
In recent years, the treatment landscape has significantly improved for patients with NSCLC, mainly due to greater understanding of the molecular biology underlying the disease and differentiation between oncogenic-addicted patients and wild-type patients [13]. Research has increasingly focused on targetable oncogenic drivers. The discovery of EGF and its receptor (EGFR), as well as its importance for cell proliferation, represented a historical landmark and led to the first targeted therapy in NSCLC [13]. The signal transduction inhibitors (EGFR TKIs) erlotinib and gefitinib act by blocking specific enzymes and growth factor receptors involved in cancer cell proliferation and, unlike the intravenous chemotherapy standard of care, they are orally administrated, which offers greater convenience for patients [12].
Despite the generally good responses to erlotinib and gefitinib seen in patients with EGF mutation-positive tumors, in some cases, they eventually developed acquired resistance and progressed [14,15]. This prompted clinical development of a second generation of EGFR TKIs. Afatinib and dacomitinib were developed with the intent of improving responses in the first-line setting and providing additional treatment options in the acquired resistance setting [15–17]. Although preclinical efficacy was encouraging, most of these alternatives were unable to overcome the acquired resistance to gefitinib and erlotinib, and third-generation EGFR TKIs are now being developed [15,16].
After the discovery of EGFR TKIs, many signaling pathways and specific oncogenic driver mutations have been identified in the NSCLC setting, including ALK mutations, KRAS mutations, MET amplifications, ROS1 rearrangements, HER2/ErbB2/neu overexpression and mutation and BRAF mutations [15,18].
Several therapies targeting ROS1 rearrangements are currently available, including crizotinib, which is an oral TKI-targeting ALK, ROS1 and MET receptors that was approved by the US Food and Drug Administration (FDA) in March 2016 and the European Medicine Agency (EMA) in August 2016 for the treatment of patients with ROS1 fusion-positive, advanced NSCLC. However, in studies of patients with ALK-positive NSCLC treated with crizotinib, the CNS was a common site of first disease progression [19]. Similarly, up to 50% of patients with ROS1 fusion-positive NSCLC treated with crizotinib develop CNS metastases during the course of their disease, and this is a major cause of morbidity [20]. Furthermore, it is estimated that 20–30% of patients with ROS1 fusion-positive NSCLC already have CNS metastases at the time of diagnosis [21]. Crizotinib is a known substrate for P-glycoprotein, a key efflux transporter of the blood–brain barrier, which means it is not able to achieve clinically relevant exposures in the CNS [22]. Therefore, an unmet need exists for a CNS-active drug for the treatment of patients with ROS1 fusion-positive NSCLC.
Entrectinib is a potent TKI of ROS1, TRKA/B/C and ALK that was specifically designed to cross the blood–brain barrier and remain in the CNS [10,11]. In a pooled analysis of three Phase I and II studies, 53 TKI-naive patients with ROS1 fusion-positive NSCLC had an ORR of 77% when treated with entrectinib. Importantly, a cohort of 20 patients with CNS metastases at baseline (per blinded independent central review [BICR]) had an intracranial ORR of 55%, demonstrating the efficacy of entrectinib in patients with CNS metastases [23,24]. Entrectinib has since been approved by the FDA in August 2019 for the treatment of ROS1 fusion-positive NSCLC and on May 29, 2020, the EMA's Committee for Medicinal Products for Human Use adopted a positive opinion for entrectinib for the treatment of adults with ROS1 fusion-positive NSCLC not previously treated with ROS1 inhibitors.
Although these promising advances have resulted in improved treatment options for patients with advanced ROS1 fusion-positive NSCLC, resistance to targeted therapies in general remains a challenge in the treatment pathway. In the future, it will be important to balance the efficacy, toxicity and costs of the different options and optimize their use as first-line single agents and/or in combination [15,18,25,26].
Methods
Samples & sources
To inform the ITCs, a systematic literature review (SLR) was required to identify all trial evidence for entrectinib and crizotinib in ROS1 fusion-positive advanced or metastatic NSCLC. It was anticipated that there would be limited trial evidence available for this population given the small number of patients; therefore, evidence for the ALK-positive population was used as a proxy when necessary, based on the similarity in the kinase domains and clinical behavior of ALK and ROS1 [27].
Systematic literature review
Two SLRs, one in ROS1 fusion-positive NSCLC and another in ALK-positive NSCLC, were conducted in accordance with PRISMA guidelines [28]. SLRs collected clinical evidence comparing the efficacy, safety and health-related quality of life (HRQoL) outcomes of entrectinib compared with crizotinib or chemotherapy. The electronic searches for the ROS1 fusion-positive SLR were conducted in October 2018 and March 2019, whereas the ALK-positive SLR was conducted in January 2017 and subsequently updated in October 2018. The searches were performed according to defined keywords in the databases Medline, Medline In-Process, Embase and Cochrane Library (CENTRAL, CDSR, DARE, HTAD) in adherence with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. Database searches were not limited by language. Clinical trials registries, Health Technology Assessment bodies and congress proceedings from the past 3 years were also included.
Primary (titles and abstracts) and secondary (full-text) screenings were conducted independently by two reviewers based on the eligibility criteria. A quality appraisal checklist, based on the criteria specified by the Centre for Reviews and Dissemination [29] and the Cochrane Library Risk of Bias tool, was used to assess publication quality of randomized controlled trials (RCTs) [30]. Non-RCTs were assessed using the Downs and Black checklist [31,32]. Electronic database search strategy and full eligibility criteria can be found in Supplementary Material 1 & 2.
Feasibility assessment & individual patient data
A study assessing the feasibility of performing an ITC of entrectinib versus crizotinib, pemetrexed plus platinum followed by pemetrexed maintenance, or chemotherapy in patients with ROS1 fusion-positive NSCLC was performed considering both clinical and methodological similarities.
To make an adjusted comparison between entrectinib patients and the comparative evidence source, individual entrectinib-treated patients were assigned statistical weights that adjust for their over- or underrepresentation relative to that observed in each comparative evidence source. Because individual patient data (IPD) are not available for the identified comparative evidence sources, pseudo-IPD data, re-created by digitizing existing curves using the GetData Graph Digitizer software (version 2.26; GetData Pty Ltd, Kogarah, Australia) [33], were considered alongside the IPD from the entrectinib trials. Individual entrectinib-treated patients were assigned statistical weights that adjust for their over- or underrepresentation relative to that observed in each comparative evidence source. Propensity weights were assigned according to the method proposed by Signorovitch [34–36]. A propensity score logistic regression model estimated the odds of being enrolled into the comparative evidence source; the model was estimated based on IPD available for the entrectinib-treated patients and published summary data available for the comparative evidence sources. As entrectinib was compared with multiple alternative treatments, one set of propensity weights was derived for each comparator study. After weighting, average baseline characteristics were balanced between the selected entrectinib cohort(s) and the comparative evidence source. Evidence for the ALK-positive population was used as a proxy when necessary [32]. This assumes that ALK versus ROS1 rearrangement status is not in itself either prognostic or a treatment-effect modifier once imbalances in other patient characteristics have been accounted for.
For the comparison of entrectinib with other alternatives, the final baseline characteristics selected for matching based on known factors were sex, Eastern Cooperative Oncology Group (ECOG) performance status 0 or 1 versus 2, smoking history, age, disease stage at enrollment (stage IIIB vs stage IV non-CNS metastases vs stage IV CNS metastases). For comparisons with crizotinib, prior treatments (treatment-naive vs prior treatment) were also considered. The percentage of CNS metastases in patients was not reported in PROFILE 1001; therefore, this value varied across three scenarios. In scenario 1, this figure was assumed to be 18.1% because this was the percentage of patients with CNS metastases as reported by Wu et al. (2018) in the Phase II crizotinib study [37] and scenario 2 assumed 24.64% of CNS metastases (as per Flatiron analyses by an internal real-world data team). Scenario 3 assumed the same percentage of CNS metastases as in the entrectinib studies, that is, 43.4% for efficacy analyses and 50% for safety analyses [38].
Data analysis
After the matching procedure was conducted and the weights derived, efficacy outcomes were compared between balanced treatment groups using statistical tests that incorporate the derived weights. For OS and PFS, weighted Kaplan–Meier curves were generated, so OS probability and PFS probability in a given length of time were obtained. Hazard ratios (HRs) comparing entrectinib cohort(s) and the comparative evidence source were estimated using weighted Cox proportional hazards models. For ORR and treatment discontinuation due to AE, odds ratios (OR) comparing entrectinib cohort(s) and the comparative evidence source were estimated using the derived weights. CI were estimated by mean of bootstrap sampling. The procedure was repeated multiple times to obtain a distribution of HRs for which the 2.5 and 97.5 percentiles were used to generate the limits of a CI.
Results
A schematic summary of the results described in this section is presented in Figure 1.

Figure 1. Schematic summary of the results described in the results.
AE: Adverse events; NSCLC: Non-small cell lung cancer; ORR: Objective response rate; OS: Overall survival; PFS: Progression-free survival.
Systematic literature review
ROS1 fusion-positive NSCLC
The database searches in the original SLR identified 1,040 citations, of which 146 were duplicates, leaving 894 references for screening. During SLR update, the database searches identified 2,676 citations, of which 219 were duplicates, leaving 2,457 references for screening. The screening procedure resulted in a final evidence base for the SLR of 61 references (Figure 2). In this SLR, no RCT was identified for the patient population of interest, and the evidence represented 11 noncomparative trials and observational studies published from 38 references.
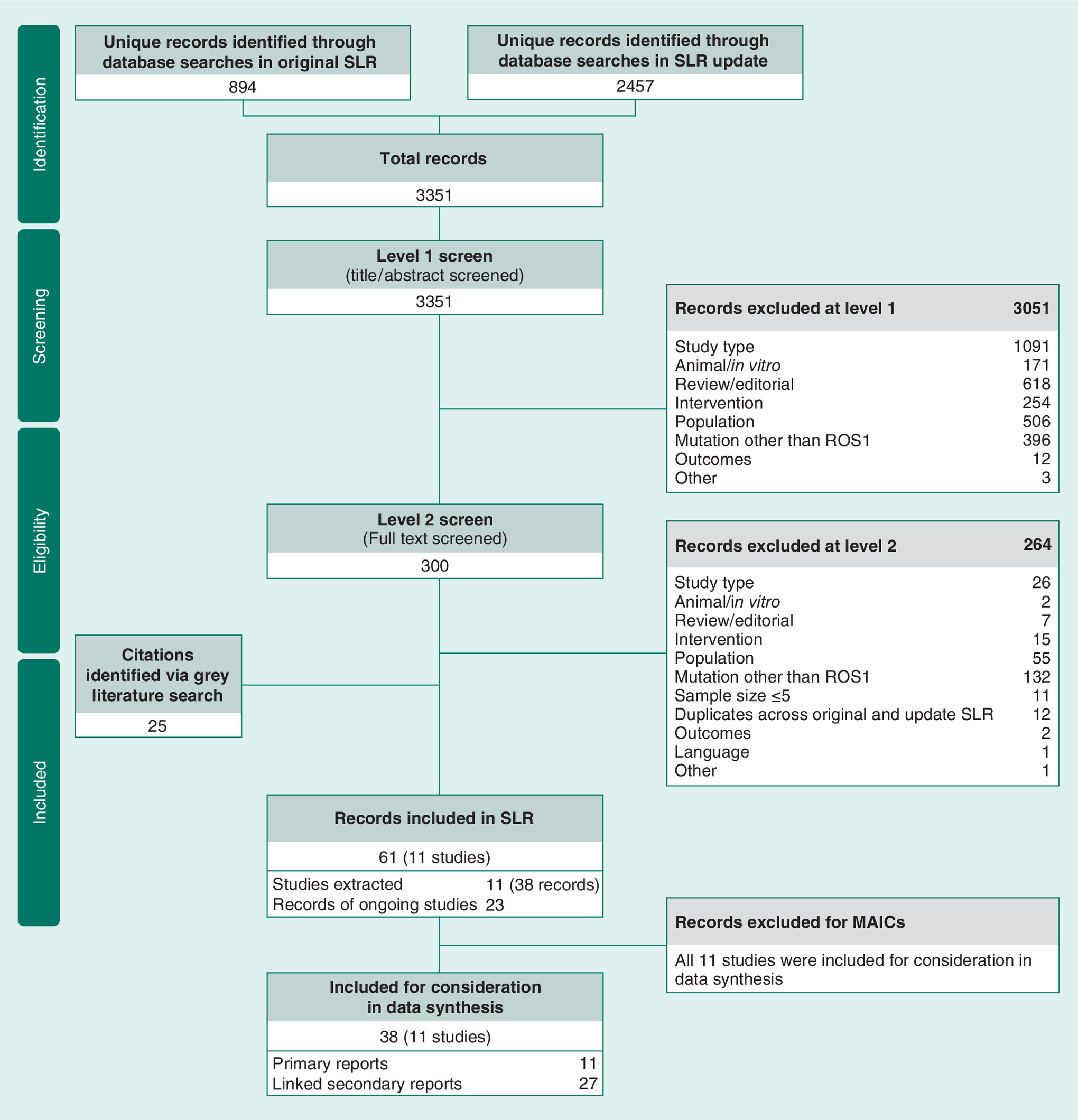
Figure 2. Diagram of ROS1 fusion-positive NSCLC SLR, in accordance with PRISMA guidelines.
NSCLC: Non-small cell lung cancer; MAIC: Matching-adjusted indirect comparison; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SLR: Systematic literature review.
ALK-positive NSCLC
The database searches identified 854 citations, of which 168 were duplicates, leaving 686 references for screening (Figure 3). The screening process resulted in a final evidence base for the systematic review of 56 references corresponding to 25 studies. After additional screening to identify studies that were relevant for consideration in the feasibility assessment for matching-adjusted indirect comparison (MAIC), the final ALK-positive NSCLC evidence base for consideration in the MAICs consisted of 20 references representative of eight studies.
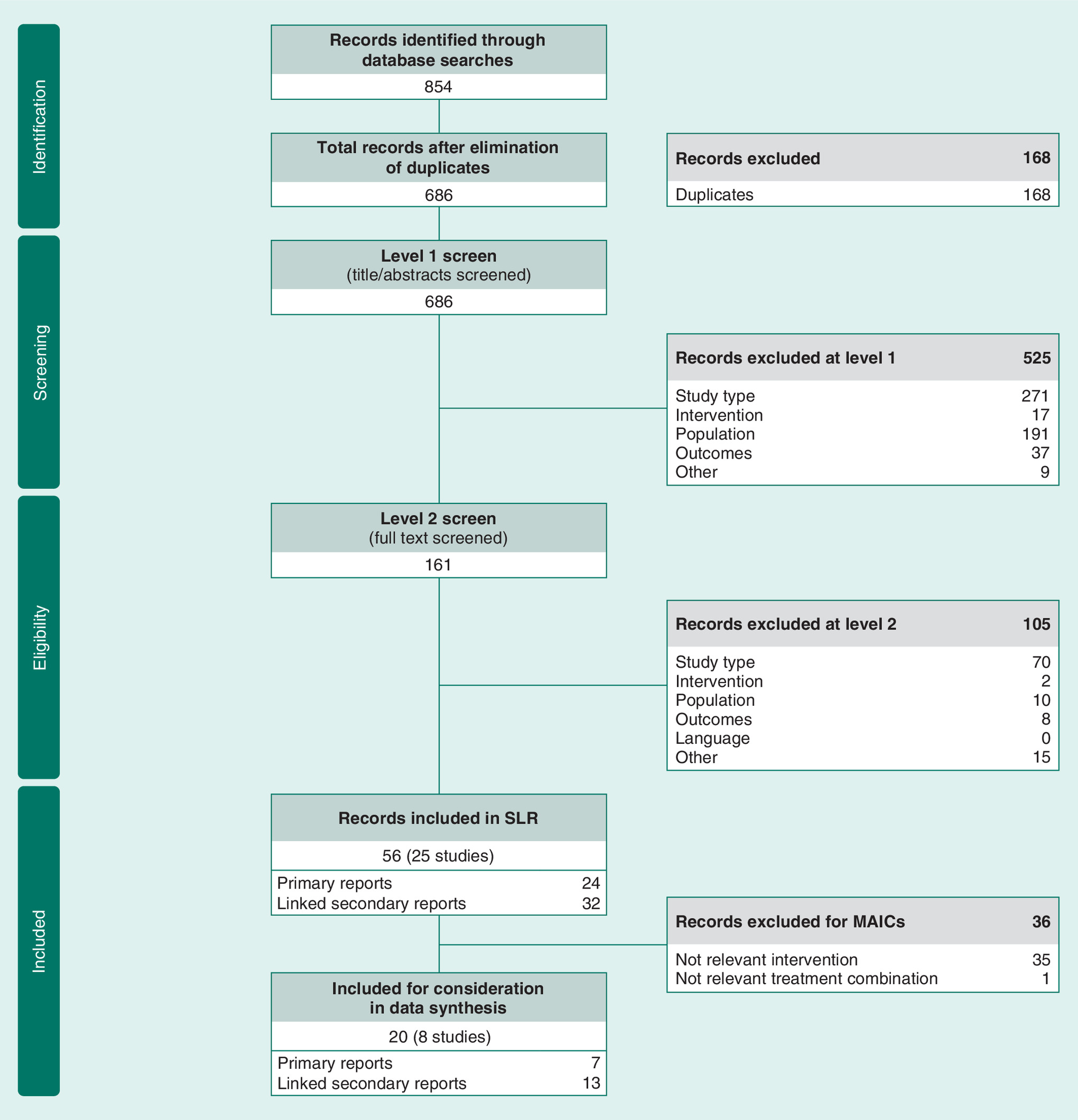
Figure 3. Diagram of ALK-positive NSCLC SLR, in accordance with PRISMA guidelines.
NSCLC: Non-small cell lung cancer; MAIC: Matching-adjusted indirect comparison; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SLR: Systematic literature review.
Indirect treatment comparison feasibility assessment
The feasibility assessment considered pooled data from three entrectinib studies (two Phase I studies – ALKA-372-001 and STARTRK-1 – and a single-arm Phase II basket study, STARTRK-2) and the studies identified in both SLRs (11 prospective studies, of which nine were parallel RCT and two were prospective single-arm studies, and eight retrospective studies). After assessment, it was concluded that it would be feasible to perform a MAIC considering the indirect comparisons suggested in Table 1. Quality assessments of the trials are presented in Supplementary Materials 3 & 4.
| Endpoint | Intervention | Intervention study | Intervention population | Comparator | Comparator study | Comparator population | Ref. |
|---|---|---|---|---|---|---|---|
| OS | Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Crizotinib | PROFILE 1001 | ROS1 NSCLC | [19] |
| Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Pemetrexed with platinum plus maintenance | ASCEND-4 | ALK+ NSCLC | [39] | |
| Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Chemotherapy (pemetrexed/docetaxel) | PROFILE 1007 | ALK+ NSCLC | [16] | |
| PFS† | Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Crizotinib | PROFILE 1001 | ROS1 NSCLC | [19] |
| PFS BICR | Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Pemetrexed with platinum plus pemetrexed maintenance | ASCEND-4 | ALK+ NSCLC | [39] |
| Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Chemotherapy (pemetrexed/docetaxel) | PROFILE 1007 | ALK+ NSCLC | [16] | |
| ORR | Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Crizotinib | PROFILE 1001 | ROS1 NSCLC | [19] |
| Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Pemetrexed with platinum plus pemetrexed maintenance | ASCEND-4 | ALK+ NSCLC | [39] | |
| Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Chemotherapy (pemetrexed/docetaxel) | PROFILE 1007 | ALK+ NSCLC | [16] | |
| Discontinuation due to AEs | Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Crizotinib | PROFILE 1001 | ROS1 NSCLC | [19] |
| Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Pemetrexed with platinum plus pemetrexed maintenance | ASCEND-4 | ALK+ NSCLC | [39] | |
| Entrectinib | Pooled entrectinib studies | ROS1 NSCLC | Chemotherapy (pemetrexed/docetaxel) | PROFILE 1007 | ALK+ NSCLC | [16] |
†
It is unclear if reported PFS for PROFILE 1001 is IA or BICR.
PROFILE 1001: clinicaltrials.gov number, NCT00585195.
ASCEND-4: clinicaltrials.gov number, NCT01828099.
PROFILE 1007: clinicaltrials.gov number, NCT00932893.
ALKA-372-001: EudraCT number, 2012-000148-88.
STARTRK-1: clinicaltrials.gov number, NCT02097810.
STARTRK-2: clinicaltrials.gov number, NCT02568267.
AE: Adverse event; BICR: Blinded independent central review; IA: Investigator assessed; NSCLC: Non-small cell lung cancer; ORR: Objective response rate; OS: Overall survival; PFS: Progression-free survival.
Indirect treatment comparison
Baseline characteristics
After matching based on the baseline factors, the weighted patient characteristics for the population of the pooled entrectinib studies were compared with each comparator study. Aggregate statistics for the entrectinib reweighted population showed that the MAIC method resulted in a patient population with equivalent characteristics to the PROFILE 1001, ASCEND-4 and PROFILE 1007 populations (Table 2).
| Comparison | Intervention | Sample size (effective sample size) | Female (%) | ECOG 2 (%) | Never smoked (%) | Age (yr) | Treatment naive (%) | Stage IV – CNS (%) | Ref. | |
|---|---|---|---|---|---|---|---|---|---|---|
| Entrectinib† vs PROFILE 1001 crizotinib‡ | Scenario 1: (assumes 18.1% CNS metastases in PROFILE 1001, as reported by Wu et al. [2018]) | Entrectinib | 53 | 64.15 | 11.32 | 58.49 | 53.55 | 13.21 | 43.40 | [37] |
| Entrectinib reweighted | 53 (34.18) | 56.60 | 1.89 | 75.47 | 55.00 | 13.21 | 18.10 | |||
| Crizotinib | 53 | 56.60 | 1.89 | 75.47 | 55.00 | 13.21 | 18.10 | |||
| Scenario 2: (assumes 24.64% CNS metastases in PROFILE 1001, as per Flatiron analyses by RWD team) | Entrectinib | 53 | 64.15 | 11.32 | 58.49 | 53.55 | 13.21 | 43.40 | ||
| Entrectinib reweighted | 53 (37.33) | 56.60 | 1.89 | 75.47 | 55.00 | 13.21 | 24.64 | |||
| Crizotinib | 53 | 56.60 | 1.89 | 75.47 | 55.00 | 13.21 | 24.64 | |||
| Scenario 3: (assumes 43.4% CNS metastases for efficacy analyses and 50% CNS metastases for safety analyses in PROFILE 1001, same percentages as in the entrectinib pooled studies) | Entrectinib | 53 | 64.15 | 11.32 | 58.49 | 53.55 | 13.21 | 43.40 | [24,38] | |
| Entrectinib reweighted | 53 (40.22) | 56.60 | 1.89 | 75.47 | 55.00 | 13.21 | 43.40 | |||
| Crizotinib | 53 | 56.60 | 1.89 | 75.47 | 55.00 | 13.21 | 43.40 | |||
| Comparison | Intervention | Sample size (effective sample size) | Female (%) | ECOG 2 (%) | Never smoked (%) | Age (yr) | Stage III-B (%) | Stage IV – CNS (%) | ||
| Entrectinib vs ASCEND-4 pemetrexed plus platinum followed by pemetrexed maintenance | Entrectinib | 53 | 64.15 | 11.32 | 58.49 | 53.55 | 5.66 | 43.40 | ||
| Entrectinib reweighted | 53 (47.50) | 60.96 | 5.88 | 65.24 | 54.00 | 2.67 | 33.16 | |||
| Pemetrexed + platinum + pemetrexed maintenance | 187 | 60.96 | 5.88 | 65.24 | 54.00 | 2.67 | 33.16 | |||
| Entrectinib vs PROFILE 1007 chemotherapy | Entrectinib | 53 | 64.15 | 11.32 | 58.49 | 53.55 | 5.66 | 43.40 | ||
| Entrectinib reweighted | 53 (36.09) | 55.17 | 8.05 | 63.79 | 49.00 | 9.20 | 34.48 | |||
| Chemotherapy | 174 | 55.17 | 8.05 | 63.79 | 49.00 | 9.20 | 34.48 | |||
†
Pooled entrectinib studies: 1 L, n = 7 (13%); 2 L, n = 3 (6%); 3 L, n = 18 (34%); 4 L, n = 6 (11%); ≥5 L, n = 19 (36%).
‡
Profile 1001 (crizotinib): 1 L, n = 7 (13%); 2 L, n = 20 (38%); 3 L, n = 13 (25%); 4 L, n = 3 (6%); ≥5 L, n = 10 (19%).
CNS: Central nervous system; ECOG: Eastern Cooperative Oncology Group; MAIC: Matching adjusted indirect comparison; RWD: Real-world data.
Overall survival
In terms of OS, results from the MAIC suggest that entrectinib may be associated with longer survival than crizotinib and chemotherapy (Table 3). In the comparison of entrectinib with crizotinib, a trend for better results could be observed in favor of entrectinib, despite the lack of statistical significance. The HR for entrectinib versus crizotinib, based on MAIC, suggests that treatment with entrectinib may reduce the risk of death compared with crizotinib in all three scenarios of CNS metastases, HRs (95% CI) were as follows: scenario 1, 0.471 (0.112–1.034); scenario 2, 0.504 (0.134–1.066); scenario 3, 0.609 (0.164–1.273).
| Endpoint | Comparator (sample size) | Comparator events n/with ORR n | Entrectinib Sum of weights | Entrectinib Events n/with ORR n | Median time to event, months (95% CI)/% with ORR | Effect size† (95% CI) | Comparator data source | Ref. |
|---|---|---|---|---|---|---|---|---|
| OS – HR | Crizotinib (53) | 16 | Scenario 1: 39.98 | 5.30 | NR (NR–NR) | 0.471 (0.112–1.034) | NICE TA529, Wu et al. (2018) | [37 40] |
| Scenario 2: 42.57 | 5.92 | NR (NR–NR) | 0.504 (0.134–1.066) | NICE TA529, Flatiron | [40] | |||
| Scenario 3: 44.91 | 7.16 | NR (NR–NR) | 0.609 (0.164–1.273) | NICE TA529, pooled entrectinib studies | [24,38,40] | |||
| Pemetrexed + platinum + pemetrexed maintenance (187) | 59 | 49.83 | 7.56 | NR (NR–NR) | 0.478 (0.167–0.918) | Soria et al. (2017) | [39] | |
| Chemotherapy (174) | 47 | 42.26 | 6.80 | NR (NR–NR) | 0.434 (0.157–0.755) | Shaw et al. (2013) | [16] | |
| PFS – HR | Crizotinib – PFS BICR (53) | 26 | Scenario 1: 39.98 | 16.39 | 26.326 (19.023–NR) | 0.939 (0.528–1.427) | NICE TA529, Wu et al. (2018) | [37,40] |
| Scenario 2: 42.57 | 17.28 | 26.316 (15.737–NR) | 0.960 (0.561–1.448) | NICE TA529, Flatiron | [40] | |||
| Scenario 3: 44.91 | 18.05 | 19.023 (15.737–NR) | 1.046 (0.640–1.603) | NICE TA529, pooled entrectinib studies | [24,38,40] | |||
| Crizotinib – PFS IA (53) | 26 | Scenario 1: 39.98 | 22.48 | 17.708 (15.507–NR) | 1.286 (0.840–1.819) | NICE TA529, Wu et al. (2018) | [37,40] | |
| Scenario 2: 42.57 | 24.32 | 17.511 (14.489–NR) | 1.346 (0.902–1.863) | NICE TA529, Flatiron | [40] | |||
| Scenario 3: 44.91 | 27.05 | 15.507 (12.222–NR) | 1.535 (1.063–2.107) | NICE TA529, pooled entrectinib studies | [24,38,40] | |||
| Pemetrexed + platinum + pemetrexed maintenance – BICR (187) | 117 | 49.83 | 21.57 | 19.023 (15.737–NR) | 0.411 (0.258–0.607) | Soria 2017 | [39] | |
| Chemotherapy (174) | 134 | 42.32 | 20.26 | 26.316 (13.635–NR) | 0.214 (0.137–0.306) | Shaw 2013 | [16] | |
| ORR – OR | Crizotinib (53) | 33 | Scenario 1: 39.98 | 32.73 | 81.86 | 2.735 (1.365–8.566) | NICE TA529, Wu et al. 2018 | [37,40] |
| Scenario 2: 42.57 | 34.63 | 81.33 | 2.641 (1.318–7.686) | NICE TA529, Flatiron | [40] | |||
| Scenario 3: 44.91 | 35.93 | 80.01 | 2.426 (1.219–7.017) | NICE TA529, pooled entrectinib studies | [24,38,40] | |||
| Pemetrexed + platinum + pemetrexed maintenance (187) | 50 | 49.83 | 40.08 | 80.44 | 11.270 (6.151–28.148) | Soria et al. 2017 | [39] | |
| Chemotherapy (174) | 34 | 43.26 | 31.73 | 73.36 | 11.337 (5.496–39.059) | Shaw et al. 2013 | [16] |
†
OS, PFS (HR) effect size <1 and ORR (OR) effect size >1 favor entrectinib over comparator.
Note: The values in bold denote results with statistical significance.
Scenario 1 assumes 18.1% CNS metastases in PROFILE 1001, as reported by Wu et al. (2018) [37]; scenario 2 assumes 24.64% CNS metastases in PROFILE 1001, as per Flatiron analyses by RWD team; scenario 3 assumes 43.4% CNS metastases for efficacy analyses and 50% CNS metastases for safety analyses in PROFILE 1001, same percentages as in the entrectinib studies [24,38].
BICR: Blinded independent central review; CNS: Central nervous system; HR: Hazard ratio; IA: Investigator assessed; NICE: National Institute for Health and Care Excellence; OR: Odds ratio; ORR: Objective response rate; OS: Overall survival; PFS: Progression-free survival; RWD: Real-world data.
In the comparison of entrectinib versus pemetrexed plus platinum followed by pemetrexed maintenance, MAIC suggests that treatment with entrectinib may be associated with a significant reduction in the risk of death compared with pemetrexed plus platinum followed by pemetrexed maintenance (HR: 0.478; 95% CI: 0.167–0.918). Lastly, when compared with chemotherapy, entrectinib may also significantly reduce the risk of death (HR: 0.434; 95% CI: 0.157–0.755).
Progression-free survival
In PROFILE 1001, it was unclear whether PFS was reported as investigator-assessed (IA) or BICR. Therefore, we performed separate comparisons of PFS data reported in PROFILE 1001 with PFS IA and PFS BICR data from the integrated entrectinib studies (Table 3). When PFS BICR was assumed, the HR was close to 1 in all three scenarios, indicating the risk of progression may be similar for both treatments. HRs (95% CI) were as follows: scenario 1, 0.939 (0.529–1.427); scenario 2, 0.960 (0.561–1.448); scenario 3, 1.046 (0.640–1.603). When PFS IA was assumed, the HR for entrectinib versus crizotinib based on MAIC suggested that treatment with entrectinib may be associated with a trend toward higher risk of disease progression relative to crizotinib; the HR (95% CI) result for scenario 3 (43.4% CNS metastases for efficacy analyses and 50.0% CNS metastases for safety analyses in PROFILE 1001) was statistically significant: scenario 1, 1.286 (0.840–1.819); scenario 2, 1.346 (0.902–1.863); scenario 3, 1.535 (1.063–2.107).
Regarding the comparison of entrectinib versus pemetrexed plus platinum followed by pemetrexed maintenance, for PFS assessed by BICR in the ASCEND-4 trial, the HR based on MAIC suggested that treatment with entrectinib may significantly reduce the risk of progression compared with pemetrexed plus platinum followed by pemetrexed maintenance (HR: 0.411; 95% CI: 0.258–0.607). This was supported by longer median PFS for patients treated with entrectinib (19 months) compared with 8 months for patients treated with pemetrexed plus platinum followed by pemetrexed maintenance.
For the same endpoint but considering the comparison with chemotherapy, the HR based on MAIC suggested that treatment with entrectinib may also significantly reduce the risk of progression (HR: 0.214; 95% CI: 0.137–0.306); this was supported by longer median PFS for patients treated with entrectinib (26.3 months) compared with 2.8 months for chemotherapy.
Kaplan–Meier plots for OS, BICR-PFS and IA-PFS with entrectinib versus scenario 1 of crizotinib (main comparator) are presented in Figure 4.
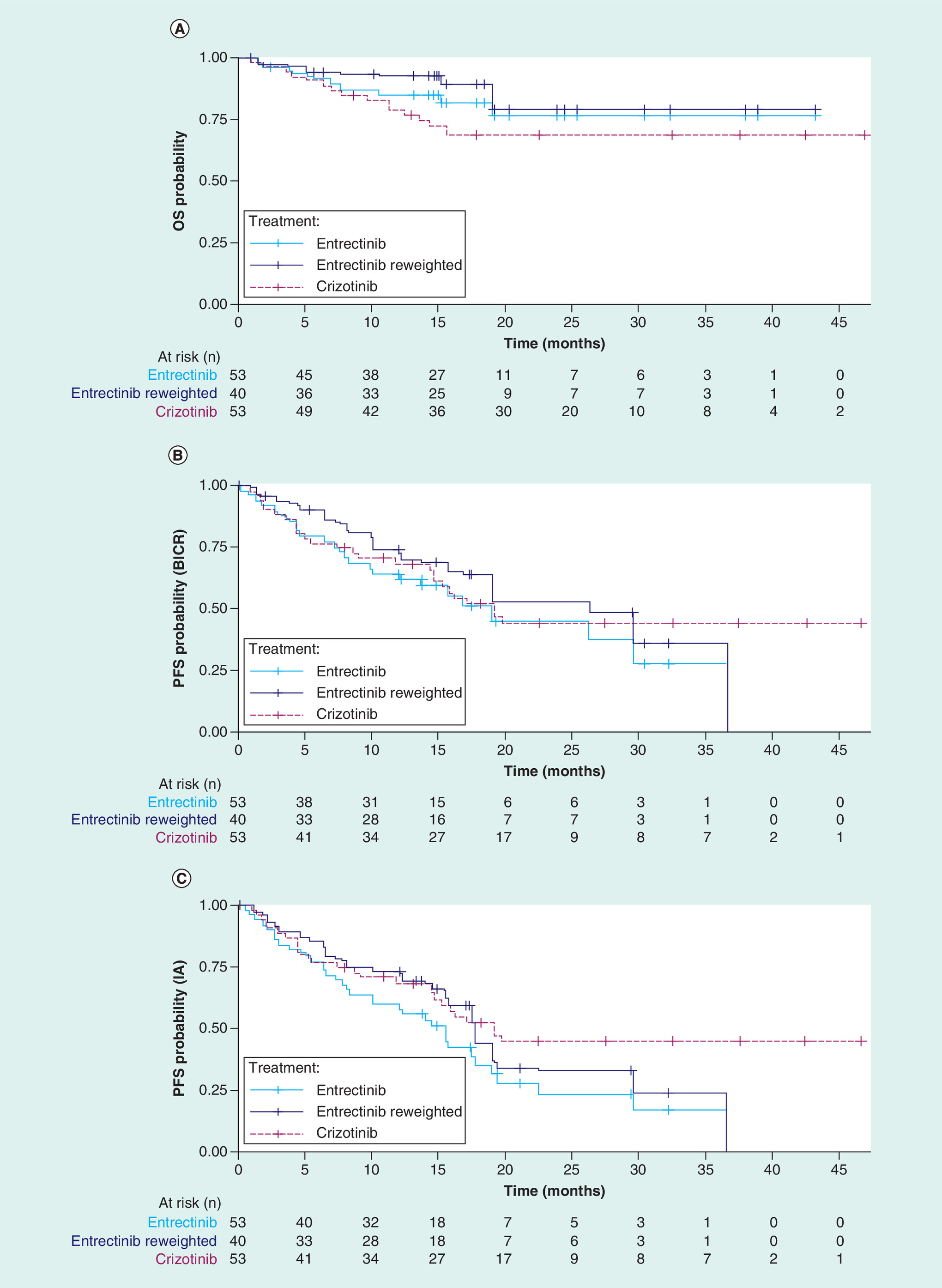
Figure 4. Kaplan–Meier plots for entrectinib versus crizotinib (main comparator) for scenario 1.
(18.1% CNS metastases – as reported by Wu et al. [2018]): (A) overall survival; (B) PFS (BICR); (C) PFS (IA).
BICR: Blinded independent central review; CNS: Central nervous system; IA: Investigator assessed; OS: Overall survival; PFS: Progression-free survival.
Objective response rate
The matching-adjusted ORR for entrectinib was significantly higher compared with crizotinib in all three scenarios of CNS metastases in PROFILE 1001 (Table 3); OR values were (95% CI): scenario 1, 2.735 (1.365–8.566); scenario 2, 2.641 (1.318–7.686); scenario 3, 2.426 (1.219–7.017). This indicates that entrectinib may be significantly more effective than crizotinib; ORR values for entrectinib versus crizotinib in the three scenarios were: scenario 1, 81 versus 62%; scenario 2, 81 versus 62%; scenario 3, 80 versus 62%.
In ASCEND 4, a significantly higher matching-adjusted ORR was seen for the entrectinib population (80%) compared with pemetrexed plus platinum followed by pemetrexed maintenance (27%). In PROFILE 1007, a higher ORR was seen for entrectinib (73%) compared with chemotherapy (20%).
Discontinuation due to adverse events
A safety population of 134 patients was used to evaluate treatment discontinuation due to AEs (Table 4). The matching-adjusted odds of discontinuation due to AEs were lower with entrectinib versus crizotinib; OR values were as follows: scenario 1, 0.896 (0.231–1.910); scenario 2, 0.874 (0.250–1.826); scenario 3, 0.793 (0.290–1.444). However, the CI around the estimated OR is wide, suggesting that the estimate is uncertain.
| Comparator (sample size) | Comparator discontinuations due to AE, n (%) | Entrectinib: Sum of weights | Entrectinib discontinuations due to AE, n (%) | OR (95% CI)† | Comparator data source | Ref. |
|---|---|---|---|---|---|---|
| Crizotinib (53) | 4 (7.54) | Scenario 1: 93.38 | 6.36 (6.81) | 0.896 (0.231–1.910) | NICE TA529, Wu 2018 | [37,40] |
| Scenario 2: 101.63 | 6.77 (6.66) | 0.874 (0.250–1.826) | NICE TA529, Flatiron | [40] | ||
| Scenario 3: 115.85 | 7.04 (6.08) | 0.793 (0.290–1.444) | NICE TA529, Pooled entrectinib studies | [24,38,40] | ||
| Pemetrexed + platinum + pemetrexed maintenance (187) | 16 (8.56) | 122.49 | 10.18 (8.31) | 0.969 (0.424–1.695) | Soria et al. (2017) | [39] |
| Chemotherapy (174) | 17 (9.77) | 114.64 | 9.93 (8.66) | 0.876 (0.383–1.618) | Shaw et al. (2013) | [16] |
†
OR <1 favors entrectinib over comparator.
AE: Adverse event; NICE: The National Institute for Health and Care Excellence; OR: Odds ratio.
The matching-adjusted OR for discontinuation of entrectinib due to AEs versus pemetrexed plus platinum followed by pemetrexed maintenance was close to 1, suggesting rates of treatment discontinuation due to AEs may be similar for both treatments (OR: 0.969; 95% CI: 0.424–1.695). A similar percentage of patients across the studies discontinued treatment due to AE (8.3% for entrectinib compared with 8.6% for pemetrexed plus platinum followed by pemetrexed maintenance). The frequency of discontinuations due to AEs was lower in the matching-adjusted entrectinib population (8.7%) than the chemotherapy population (9.8%), although the result was not statistically significant.
Discussion
The overall aim of this study was to evaluate the evidence base and, if feasible, to perform ITCs to estimate relevant treatment effects of entrectinib compared with alternative treatments for patients with ROS1 fusion-positive NSCLC. Crizotinib was the main comparator of interest for these analyses but alternative NSCLC treatments such as pemetrexed plus platinum chemotherapy followed by pemetrexed maintenance and pemetrexed monotherapy or docetaxel monotherapy, were also considered.
Due to the rarity of the ROS1 gene fusion, no head-to-head studies directly comparing entrectinib with crizotinib or any other alternative treatment have been performed, and an ITC using a propensity score methodology was necessary to compare the treatments. This methodology allowed us to balance baseline demographic and clinical characteristics across the treatment groups and to reduce bias in the comparison. This study represents a comprehensive assessment of the benefit of entrectinib versus crizotinib and other alternatives and, with the infeasibility of RCTs in this population, provides a good basis to assess the effectiveness of entrectinib versus other potential treatment options in patients with ROS1 fusion-positive NSCLC.
The evidence base for the ITCs was derived from two SLRs: one for the ROS1 fusion-positive NSCLC population and another for the ALK-positive NSCLC population. Because no data were found in the ROS1 fusion-positive NSCLC population in comparison with chemotherapy, ALK-positive information was used. ALK-positive data have been considered a proxy for ROS1 population data for several reasons [32]: the kinase domains of ALK and ROS1 share 77% of amino acids in the ATP-binding sites, ALK-positive and ROS1 fusion-positive advanced NSCLC are similar in terms of clinical behavior, proxy use has been accepted by the EMA in similar contexts, and the approach has been validated by clinical experts.
For the matching procedure, all predictive and prognostic factors were assessed, and all relevant ones were included to limit the risk of bias in the estimates. Nonetheless, it should be noted that both PROFILE 1007 and ASCEND-4 enrolled patients with ALK-positive NSCLC rather than patients with ROS1 fusion-positive NSCLC, the population that is the primary focus of these analyses. Because there is no overlap between the study populations in terms of ALK versus ROS1 rearrangement status, this could not be included in the matching process and required the assumption that ALK versus ROS1 rearrangement status is not in itself either prognostic or a treatment effect modifier once imbalances in other patient characteristics have been accounted for. After the matching procedure was completed, the sample size was reduced to the effective sample size, but this reduction was not large, which shows that there is no cause for concern about the reliability of the results. In general, the matching procedure was considered successful.
Overall, the ITC suggests that there is a trend for improved results in favor of entrectinib in relation to all three comparators. The matching-adjusted entrectinib group was found to have significantly better ORR relative to crizotinib in all three scenarios. ORs in the three scenarios ranged from 2.43 (95% CI: 1.37–8.57) to 2.74 (95% CI: 1.22–7.02). Similar results were found in comparison with pemetrexed plus platinum followed by pemetrexed maintenance (OR: 11.27 [95% CI: 6.15–28.15]), and versus chemotherapy (OR: 11.34 [95% CI: 5.50–39.06]). Upon matching adjustment, entrectinib showed improved OS compared with crizotinib, but the differences were not statistically significant in any of the three scenarios. Entrectinib may significantly improve OS compared with pemetrexed plus platinum followed by pemetrexed maintenance (HR: 0.48; 95% CI: 0.17–0.92) and chemotherapy (HR: 0.43; 95% CI: 0.16–0.76).
It was unclear whether the PFS reported in PROFILE 1001 was assessed by BICR or IA [19], and therefore separate comparisons of PFS per BICR and PFS per IA data from the integrated entrectinib studies with the PFS data reported in PROFILE 1001 were performed. Additional data or future reporting can confirm whether PFS data in PROFILE 1001 was indeed blinded or IA. Using three scenario analyses, entrectinib and crizotinib yielded similar HRs for PFS, irrespective of whether BICR or IA was assumed, with the exception of one calculation (scenario 3 with PFS IA), which suggests worse performance with entrectinib versus crizotinib. However, comparing different trials without patient-level data requires assumptions to be made around characteristics and their weighting in propensity score matching; this therefore limits the inferences that can be drawn from the results. In our analyses, the proportion of patients with CNS metastases in the crizotinib trial was an unknown factor that disproportionately influenced the outcome of the calculations; high assumed proportions of CNS metastases in the crizotinib study would result in a high estimated performance of crizotinib in the CNS, based on fixed or known outcomes of the trial. Crizotinib has been reported to have limited intracranial efficacy [22]; as a consequence, such a result may not reflect the true clinical situation.
Another point of note is that although PFS results were generally similar across treatments (with the single noted exception), in this analysis we found that OS data favored entrectinib. This contrasts with prior reports in which little difference was observed in OS between EGFR TKIs and chemotherapy, despite significant improvements in PFS [41,42]. OS remains the gold standard endpoint for many cancer clinicians and patients [43,44], and therefore the estimated superiority of entrectinib versus crizotinib regarding OS is interesting, particularly for a patient population with few therapeutic options.
In terms of limitations for this study, the low prevalence of ROS1 fusion-positive NSCLC resulted in a small sample size for analysis, and given the paucity and relative immaturity of data, with few events observed, there is some inherent uncertainty in the results; this is reflected in wide CIs in the estimation of relative effect sizes. There may also be the potential for residual confounding from prognostic factors or treatment effect modifiers with little or no overlap between studies. For example, the integrated entrectinib dataset included only 17 patients treated in the first line, [24] and it was therefore not possible to match based on line of treatment in the comparisons of entrectinib with ASCEND-4 pemetrexed and platinum followed by pemetrexed maintenance. However, by matching based on other baseline characteristics, this may still have been accounted for indirectly, as we would expect line of treatment to correlate with other disease characteristics. Similarly, it was not possible to match patients based on disease histology due to missing information for some patients in the entrectinib dataset.
With the approval of entrectinib for the treatment of ROS1 fusion-positive NSCLC, patients have another treatment option, representing an advance in the management of the disease but also an additional decision for doctors, payers and health technology assessment agencies. Given the lack of direct comparative data due to the rarity of the disease and the unfeasibility of RCTs, it is difficult for decision-makers to make informed decisions on the best choice of treatment. The results of this study could help to inform that decision by providing evidence of the relative treatment effects of entrectinib compared with the standard of care in this population. Although the results presented in this study support the value of entrectinib as an innovative treatment for patients with ROS1 fusion-positive NSCLC, further analyses comparing entrectinib with the standard of care as well as the inclusion of registry data are needed to better translate the value of entrectinib in the clinical practice.
Conclusion
In recent years, the growth of precision oncology and application of precision TKIs has changed the approach to treatment of NSCLC and the management strategy used with these patients, especially those with advanced disease. TKIs currently represent the evidence-based standard of care for this type of cancer and entrectinib, a potent TKI, is an emerging and promising alternative for treatment of patients with ROS1 fusion-positive NSCLC, as supported by the findings of this study. This analysis suggests that entrectinib may improve OS and significantly increase ORR relative to crizotinib with no or minor differences in terms of PFS and treatment discontinuations. Compared with pemetrexed plus platinum followed by pemetrexed maintenance and chemotherapy, this analysis is consistent with entrectinib being associated with improved OS, PFS and ORR. The results support the potential of entrectinib as a new treatment for patients with ROS1 fusion-positive NSCLC, including patients with CNS metastases.
•
Because of the rarity of the ROS1 gene fusion, only single-arm studies have been conducted for entrectinib, and to date, no head-to-head study has directly compared entrectinib with crizotinib.
•
The aim of this analysis was to estimate relative treatment effects of entrectinib, a potent inhibitor of TRKA/B/C and ROS1, versus alternative treatments approved for use in ROS1 fusion-positive (ROS1+) non-small cell lung cancer (NSCLC).
•
Published studies on entrectinib and the comparators of interest, crizotinib, pemetrexed plus platinum followed by pemetrexed maintenance, and chemotherapy (docetaxel monotherapy and pemetrexed monotherapy), were identified by a systematic literature review.
•
Matching adjusted indirect comparison (MAIC) of the studies was performed; matching was based on known prognostic/predictive factors. Three scenario analyses were performed to account for variation/nonreporting of the proportion of patients with central nervous system (CNS) metastases.
•
Indirect treatment comparisons were performed for the outcomes objective response rate (ORR), overall survival (OS), progression-free survival (PFS) and discontinuation due to adverse events (AE).
•
Overall, entrectinib was associated with a trend for improved results in relation to all three treatment comparators.
•
In all three scenarios, the matching-adjusted entrectinib group had significantly better ORR (odds ratio ranging from 2.43 to 2.74) and numerically favorable OS (hazard ratio: 0.47 to 0.61) and AE-related discontinuation rates (odds ratio: 0.79 to 0.90) versus crizotinib.
•
In comparisons with pemetrexed plus platinum followed by pemetrexed maintenance and chemotherapy, entrectinib treatment yielded higher OS, PFS and ORR.
•
This analysis suggests that entrectinib may improve OS and significantly increase ORR relative to crizotinib with no or minor differences in terms of PFS and treatment discontinuations.
•
These results support the potential of entrectinib as an efficacious new treatment for patients with ROS1 fusion-positive NSCLC, including patients with CNS metastases.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
All authors were involved in the development of this manuscript and approved its submission. P Chu participated in the planning and design of the systematic literature review (SLR). M Antoniou and M Daigl were responsible for the statistical analyses presented in this study. A Aziez provided medical input. MK Bhutani was responsible for planning and conducting the SLR.
Acknowledgments
The authors thank the patients treated with crizotinib whose real-world data contributed to this study, as well as the patients, their families and the participating study centers from the entrectinib clinical trials. We also acknowledge the valuable contribution of Luisa Quieros to this manuscript.
Financial & competing interests disclosure
This study was funded by F. Hoffmann-La Roche Ltd. P Chu, M Antoniou, A Aziez and M Daigl are employees of F. Hoffmann-La Roche Ltd. MK Bhutani was an employee of BresMed and received funding from F. Hoffmann-La Roche Ltd at the time of conducting this review; MK Bhutani did not receive payment to author this publication. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Third-party medical writing assistance, under the direction of the authors, was provided by Laura Vergoz, PhD, of Gardiner-Caldwell Communications and was funded by F. Hoffmann-La Roche Ltd.
Data sharing statement
Qualified researchers may request access to individual patient–level data through the clinical study data request platform (https://vivli.org/). Further details on Roche's criteria for eligible studies are available here (https://vivli.org/members/ourmembers/). For further details on Roche's Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm.
Open Access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 145.29 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J. Clin. 65(2), 87–108 (2015).
2.
Planchard D, Popat S, Kerr K et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 30(5), 863–870 (2019).
3.
Vaishnavi A, Le AT, Doebele RC. TRKing down an old oncogene in a new era of targeted therapy. Cancer Discov. 5(1), 25–34 (2015).
4.
Zugazagoitia J, Molina-Pinelo S, Lopez-Rios F, Paz-Ares L. Biological therapies in nonsmall cell lung cancer. Eur. Respir. J. 49(3), 1601520 (2017).
5.
Clave S, Gimeno J, Munoz-Marmol AM et al. ROS1 copy number alterations are frequent in non-small cell lung cancer. Oncotarget 7(7), 8019–8028 (2016).
6.
Scheffler M, Schultheis A, Teixido C et al. ROS1 rearrangements in lung adenocarcinoma: prognostic impact, therapeutic options and genetic variability. Oncotarget 6(12), 10577–10585 (2015).
7.
Gou LY, Niu FY, Wu YL, Zhong WZ. Differences in driver genes between smoking-related and non-smoking-related lung cancer in the Chinese population. Cancer 121(Suppl. 17), 3069–3079 (2015).
8.
Facchinetti F, Rossi G, Bria E et al. Oncogene addiction in non-small cell lung cancer: focus on ROS1 inhibition. Cancer Treat. Rev. 55, 83–95 (2017).
9.
Dong J, Li B, Lin D, Zhou Q, Huang D. Advances in targeted therapy and immunotherapy for non-small cell lung cancer based on accurate molecular typing. Front. Pharmacol. 10(230), 230 (2019).
10.
Fischer H, Ullah M, De La Cruz C et al. Entrectinib, a TRK/ROS1 inhibitor with anti-CNS tumor activity: differentiation from other inhibitors in its class due to weak interaction with P-glycoprotein. Neuro-Oncol. 22 (6), 819–829 (2020).
11.
Menichincheri M, Ardini E, Magnaghi P et al. Discovery of entrectinib: a new 3-aminoindazole as a potent anaplastic lymphoma kinase (ALK), c-ros oncogene 1 kinase (ROS1), and pan-tropomyosin receptor kinases (Pan-TRKs) inhibitor. J. Med. Chem. 59(7), 3392–3408 (2016).
12.
Coccia M. Path-breaking target therapies for lung cancer and a far-sighted health policy to support clinical and cost effectiveness. Health Pol. Technol. 3, 74–82 (2014).
13.
Morabito A. The evolution of the treatment of advanced NSCLC. Recenti Progressi Medicina 107(10), 510–514 (2016).
14.
Yu HA, Riely GJ. Second generation epidermal growth factor receptor tyrosine kinase inhibitors in lung cancers. J. Natl. Compr. Canc. Netw. 11(2), 161–169 (2013).
15.
Chan BA, Hughes BGM. Targeted therapy for non-small cell lung cancer: current standards and the promise of the future. Transl. Lung Cancer Res. 4(1), 36–54 (2015).
16.
Shaw AT, Kim DW, Nakagawa K et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N. Engl. J. Med. 368(25), 2385–2394 (2013).
• Crizotinib demonstrated a superior efficacy to standard chemotherapy in 347 patients with locally advanced or metastatic ALK-positive lung cancer who had received one prior platinum-based regimen.
17.
Karachaliou N, Fernandez-Bruno M, Bracht JWP, Rosell R. EGFR first- and second-generation TKIs—there is still place for them in EGFR-mutant NSCLC patients. Transl. Cancer Res. 8(Suppl. 1), 23–47 (2019).
18.
Russo A, Lopes AR, Mccusker MG et al. New targets in lung cancer (excluding EGFR, ALK, ROS1). Curr. Oncol. Rep. 22(5), 48 (2020).
19.
Shaw AT, Ou SH, Bang YJ et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N. Engl. J. Med. 371(21), 1963–1971 (2014).
• In a Phase I study expansion cohort, crizotinib showed marked antitumor activity (overall response rate 72.0%; median progression-free survival 19.2 months; median duration of response 17.6 months) in patients with advanced ROS1-rearranged non-small cell lung cancer.
20.
Ou SI, Zhu VW. CNS metastasis in ROS1+ NSCLC: An urgent call to action, to understand, and to overcome. Lung Cancer 130, 201–207 (2019).
21.
Patil T, Smith DE, Bunn PA et al. The incidence of brain metastases in stage IV ROS1-rearranged non-small cell lung cancer and rate of central nervous system progression on crizotinib. J. Thorac. Oncol. 13(11), 1717–1726 (2018).
• Retrospective analysis of patients with stage IV ROS1 fusion-positive non-small cell lung cancer treated with crizotinib. More than a third (36%) of treatment-naive patients had central nervous system (CNS) metastases at diagnosis, and the CNS was the first and sole site of progression in 47% of patients on crizotinib treatment.
22.
Peters S, Camidge DR, Shaw AT et al. Alectinib versus crizotinib in untreated ALK-positive non-small-cell lung cancer. N. Engl. J. Med. 377(9), 829–838 (2017).
23.
Doebele R, Ahn M, Siena S et al. OA02.01 Efficacy and safety of entrectinib in locally advanced or metastatic ROS1 fusion-positive non-small cell lung cancer (NSCLC). J. Thorac. Oncol. 13(10), S321–S322 (2018).
24.
Drilon A, Siena S, Dziadziuszko R et al. Entrectinib in ROS1 fusion-positive non-small-cell lung cancer: integrated analysis of three Phase 1–2 trials. Lancet Oncol. 21(2), 261–270 (2020).
•• Entrectinib showed clinically meaningful (overall response rate 77.4%; median progression-free survival 19.0 months) and durable (median duration of response 24.6 months) efficacy in patients with ROS1 fusion-positive non-small cell lung cancer and was well tolerated with a manageable safety profile.
25.
Macfarland SP, Naraparaju K, Iyer R et al. Mechanisms of entrectinib resistance in a neuroblastoma xenograft model. Mol. Cancer Ther. 19(3), 920–926 (2020).
26.
Ku BM, Bae YH, Lee KY et al. Entrectinib resistance mechanisms in ROS1-rearranged non-small cell lung cancer. Invest. New Drugs 38, 360–368 (2020).
27.
National Institute for Health and Care Excellence (NICE). TA 529: Crizotinib for treating ROS1-positive advanced non-small-cell lung cancer (2018). www.nice.org.uk/guidance/ta529.
28.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339, b2535 (2009).
29.
CRD's guidance for undertaking reviews in health care (2018). www.york.ac.uk/media/crd/Systematic_Reviews.pdf
30.
The Cochrane Collaboration Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011] (2011). www.handbook.cochrane.org
31.
Downs S, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Commun. Health 52(6), 377–384 (1998).
32.
TA 529: Crizotinib for treating ROS1-positive advanced non-small-cell lung cancer (2018). www.nice.org.uk/guidance/ta529 .
33.
Fedorov S. GetData Graph Digitizer version 2.26 (2020). www.getdata-graph-digitizer.com/
34.
Signorovitch JE, Wu EQ, Yu AP et al. Comparative effectiveness without head-to-head trials. PharmacoEconomics 28(10), 935–945 (2010).
35.
Signorovitch JE, Sikirica V, Erder MH et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health 15(6), 940–947 (2012).
36.
Rosenbaum PR, RD B. The central role of the propensity score in observational studies for causal effects. Biometrika 70(1), 41–55 (1983).
37.
Wu YL, Yang JCH, Kim DW et al. Phase II study of crizotinib in east asian patients with ROS1-positive advanced non-small-cell lung cancer. J. Clin. Oncol. 36(14), 1405–1411 (2018).
•• In this Phase II study, crizotinib demonstrated clinically meaningful benefit (overall response rate 71.7%; median progression-free survival 15.9 months) and durable responses (median duration of response 19.7 months) in East Asian patients with ROS1-positive advanced non-small cell lung cancer.
38.
Drilon A, Barlesi F, De Braud F et al. Entrectinib in locally advanced or metastatic ROS1 fusion-positive non-small cell lung cancer (NSCLC): Integrated analysis of ALKA-372-001, STARTRK-1 and STARTRK-2. Cancer Res. 79, Abst. n CT192 (2019).
•• In an integrated analysis of three Phase I/II trials, entrectinib was tolerable with a manageable safety profile and demonstrated efficacy (overall response rate 77.4%; median progression-free survival 19.0 months) in patients with ROS1 fusion-positive non-small cell lung cancer.
39.
Soria J-C, Tan DSW, Chiari R et al. First-line ceritinib versus platinum-based chemotherapy in advanced ALK-rearranged non-small-cell lung cancer (ASCEND-4): a randomised, open-label, Phase 3 study. Lancet 389(10072), 917–929 (2017).
• In this randomized, open-label, Phase III study, ceritinib showed a statistically significant improvement in median progression-free survival (16.6 months) versus chemotherapy (8.1 months; hazard ratio: 0.55; p < 0.00001) in untreated patients with stage IIIB/IV ALK-rearranged non-small cell lung cancer.
40.
Ou SH, Janne PA, Bartlett CH et al. Clinical benefit of continuing ALK inhibition with crizotinib beyond initial disease progression in patients with advanced ALK-positive NSCLC. Ann. Oncol. 25(2), 415–422 (2014).
• Patients with advanced ALK-positive non-small cell lung cancer who continued crizotinib treatment beyond progression had a longer overall survival and showed higher rates of Eastern Cooperative Oncology Group PS 1/2 than those who did not continue crizotinib beyond progression.
41.
Fenchel K, Sellmann L, Dempke WC. Overall survival in non-small cell lung cancer-what is clinically meaningful? Transl. Lung Cancer Res. 5(1), 115–119 (2016).
42.
Hamada T, Kosumi K, Nakai Y, Koike K. Surrogate study endpoints in the era of cancer immunotherapy. Ann. Transl. Med. 6(Suppl. 1), S27 (2018).
43.
Wu YL, Zhou C, Liam CK et al. First-line erlotinib versus gemcitabine/cisplatin in patients with advanced EGFR mutation-positive non-small-cell lung cancer: analyses from the Phase III, randomized, open-label, ENSURE study. Ann. Oncol. 26(9), 1883–1889 (2015).
44.
Li Y, Appius A, Pattipaka T, Feyereislova A, Cassidy A, Ganti AK. Real-world management of patients with epidermal growth factor receptor (EGFR) mutation-positive non-small-cell lung cancer in the USA. PLoS ONE 14(1), e0209709 (2019).
Information & Authors
Information
Published In
Pages: 861 - 876
PubMed: 32648475
Copyright
© 2020 Paula Chu. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 24 April 2020
Accepted: 16 June 2020
Published online: 10 July 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Matching-adjusted indirect comparison: entrectinib versus crizotinib in ROS1 fusion-positive non-small cell lung cancer. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0063
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Misako Nagasaka, Geoffrey Liu, Maurice Pérol, Wenfeng Chen, Lyudmila Bazhenova, Caicun Zhou, Comparative efficacy of taletrectinib versus first-generation TKIs in TKI-naïve ROS1+ non-small cell lung cancer: A matching-adjusted indirect comparison, Lung Cancer, 10.1016/j.lungcan.2026.109538, 219, (109538), (2026).
- Nadia Karim, David Waterhouse, Simon Jones, Björn Stollenwerk, Cost-effectiveness of sotorasib versus adagrasib in previously treated KRAS G12C-mutated advanced NSCLC: a US healthcare payer perspective , Journal of Medical Economics, 10.1080/13696998.2025.2604968, 29, 1, (77-92), (2026).
- Divyan Chopra, Zhiyi Lan, David M. Waterhouse, Jürgen Wolf, Enriqueta Felip, Hoora Moradian, Nadia Karim, Cynthia Obiozor, Björn Stollenwerk, Matching-Adjusted Indirect Comparison of Sotorasib Versus Adagrasib in Previously Treated Advanced/Metastatic Non-Small Cell Lung Cancer Harboring KRAS G12C Mutation, Advances in Therapy, 10.1007/s12325-025-03259-8, 42, 9, (4300-4317), (2025).
- Jürgen Wolf, Sarah Goring, Adam Lee, Byoung Chul Cho, Alexander Drilon, Yong Yuan, Dieter Ayers, Greta Lozano-Ortega, Ellen E. Korol, Sarah G. Korpach, Madeleine Crabtree, Lavanya Huria, Christophe Y. Calvet, D. Ross Camidge, Population-Adjusted Indirect Treatment Comparisons of Repotrectinib Among Patients with ROS1+ NSCLC, Cancers, 10.3390/cancers17050748, 17, 5, (748), (2025).
- Yongfeng Yu, Yun Fan, Xiaorong Dong, Juan Li, Yan Yu, Jun Zhao, Sha Tao, Yujun Chen, Mo Chen, Yueming Liu, Jiahui Xu, Qiaonan Zhu, Xichun Hu, Shun Lu, Entrectinib versus crizotinib in Asian patients with ROS1-positive non-small cell lung cancer: A matching-adjusted indirect comparison, Lung Cancer, 10.1016/j.lungcan.2024.108018, 198, (108018), (2024).
- Monica Daigl, Seye Abogunrin, Felipe Castro, Sarah F McGough, Rachele Hendricks Sturrup, Cornelis Boersma, Keith R Abrams, Advancing the role of real-world evidence in comparative effectiveness research, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0101, 13, 12, (2024).
- Ibrahim M. Abbass, Daniel M. Sheinson, Anuj Shah, Adam Gondos, Sarika Ogale, Cost-effectiveness of large-panel next-generation sequencing in guiding first-line treatment decisions for patients with nonsquamous advanced non–small cell lung cancer, Journal of Managed Care & Specialty Pharmacy, 10.18553/jmcp.2024.30.7.649, 30, 7, (649-659), (2024).
- Nalan Akyürek, Molecular Carcinogenesis of Lung Cancer, Airway Diseases, 10.1007/978-3-031-22483-6_59-1, (1011-1031), (2023).
- Essam A. Ali, Muzaffar Iqbal, Gamal A. E. Mostafa, Rashad Al Salahi, Development and Validation of an Ecofriendly, Rapid, Simple and Sensitive UPLC-MS/MS Method for Entrectinib Quantification in Plasma for Therapeutic Drug Monitoring, Separations, 10.3390/separations10090494, 10, 9, (494), (2023).
- Brigida Stanzione, Alessandro Del Conte, Elisa Bertoli, Elisa De Carlo, Alberto Revelant, Michele Spina, Alessandra Bearz, Therapeutical Options in ROS1—Rearranged Advanced Non Small Cell Lung Cancer, International Journal of Molecular Sciences, 10.3390/ijms241411495, 24, 14, (11495), (2023).